Stopping measles in its tracks
The AFT supports public health efforts to keep children and our communities safe. A new measles outbreak is a stark reminder that childhood immunizations are essential to spare children from serious infectious diseases. The Centers for Disease Control and Prevention (CDC) and state health departments have issued a health advisory for the multistate outbreak of measles associated with travel to Disneyland in California. Educators and school staff can play an important role in stopping this outbreak if it spreads to their communities.
What does it mean to have the measles?
- Measles is a highly contagious acute viral respiratory illness. It is characterized by fever (with temperatures as high as 105 degrees Fahrenheit) and malaise, cough, runny nose and conjunctivitis (pink eye), followed by a rash.
- The rash usually appears about 14 days after a person is exposed; however, the incubation period ranges from seven to 21 days.
- The rash spreads from the head to the trunk to the lower extremities.
- Infected people are contagious from four days before their rash starts through four days afterward.
- Measles can cause severe health complications, including pneumonia, encephalitis and death.
- Measles is transmitted by contact with an infected person through coughing and sneezing.
- After an infected person leaves a location, the virus remains viable for up to two hours on surfaces and in the air.
Should we be worried?
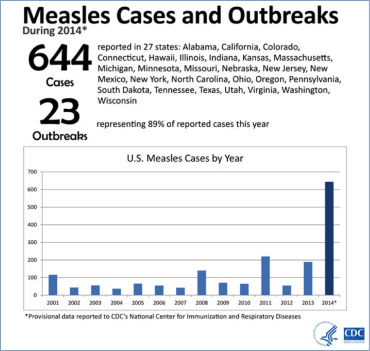
A measles outbreak started in California in December 2014. Fifty-one total cases have been reported to the CDC, with an eastward-moving spread from Disneyland to six states and Mexico, including Utah (three cases), Washington (two), Oregon (one), Colorado (one), Nebraska (one) and Arizona (one). In 2014, cases related to different sources were reported in 22 other states.
This disease was declared eliminated from the United States in 2000 because Americans achieved incredibly high immunity by adhering to recommendations to get the MMR (measles, mumps and rubella) vaccine. However, it is still common in other countries. The virus is highly contagious and can spread rapidly in areas where people are not vaccinated. The number of cases and outbreaks identified in 2014 is much higher than in recent previous years.
A couple of details in recent history make this current reintroduction of measles particularly significant:
- Many young pediatricians and healthcare workers have no experience with the disease; and
- In some communities, significant numbers of children are not vaccinated. This is due in some cases to parents’ beliefs and preferences; low vaccination adherence is also related to access to the vaccine and healthcare providers who offer it during family-friendly times.
AFT members have an important role to play in responding to this outbreak, preventing its spread and preventing future outbreaks
- Schools and districts need to increase education and information campaigns that help families and children understand the risks related to measles and local immunization requirements [search state policies].
- Awareness and prevention education should include a discussion of the value of the vaccine both at and beyond school. For example, as families with unvaccinated children think ahead toward spring break vacations, they may want to consider whether their children will be exposed to a possible case, such as at Disneyland or another place where children—and possibly unvaccinated children—are concentrated.
- California has developed template letters in English and Spanish for schools that need to communicate with families about a confirmed case.
- Anyone who works with and for high-risk populations should make sure that they have documented evidence of immunity. School personnel should be vaccinated because young children and babies are more prone to illness as their immunity develops. Also, children are less likely to practice good hygiene (for example, washing their hands, covering their mouth when they cough and using tissues) and are more likely to expose you to their bodily fluids. Some infectious diseases, like the measles, can be very serious and highly infectious several days before any symptoms appear.
High-risk populations include:
- Infants and children under age 5;
- Adults over age 20;
- Pregnant women; and
- People with compromised immune systems, such as from leukemia, HIV infection and/or cancer treatment.
Evidence of immunity includes at least one of the following:
- Written documentation of adequate vaccination:
- One or more doses of a measles-containing vaccine administered on or after the first birthday for preschool-age children and adults not at high risk; or
- Two doses of measles-containing vaccine for school-age children and adults at high risk, including college students, healthcare personnel and international travelers.
- Laboratory evidence of immunity.
- Laboratory confirmation of measles.
- Birth in the United States before 1957.
- Schools and districts should coordinate with local health departments, pharmacies and/or clinics to improve access to the vaccine, especially for families without or between insurance coverage, low-income families, and families in which all caregivers or guardians work during the day.
The New York State Education Department has developed guidelines on organizing a vaccination clinic with and in schools.
- Schools and districts with high percentages (above 4 percent) of students without evidence of immunity should develop a clear policy that explains what they will do when an index case is identified. Examples of policies are shared below:
- Nebraska bans children who do not provide documentation of immunization.
- Utah bans children who do not provide documentation of both doses of the vaccine.
- Texas bans children diagnosed with measles from school until four days after their rash is no longer apparent.
- Washington allows children to be conditionally enrolled without up-to-date vaccinations for up to one year, then reserves the right to exclude them from school.
Many states allow families to file religious and personal belief exemptions from vaccinations. For jurisdictions interested in increasing adherence, there is some evidence that policies requiring a doctor’s signature along with personal belief exemption paperwork are effective.
Getting the MMR vaccine
Children
The CDC recommends that all children get two doses of the MMR vaccine, starting with the first dose at 12 to 15 months of age, and the second dose at 4 to 6 years of age. Children can receive the second dose earlier as long as it is at least 28 days after the first dose.
Students at post–high school educational institutions
Students at post–high school educational institutions who do not have evidence of immunity against measles need two doses of the MMR vaccine, separated by at least 28 days.
Adults
Adults who do not have evidence of immunity against measles should get at least one dose of the MMR vaccine.
Healthcare personnel
Healthcare personnel should have documented evidence of immunity against measles, according to the recommendations of the Advisory Committee on Immunization Practices. Healthcare personnel without evidence of immunity should get two doses of the MMR vaccine, separated by at least 28 days.